

Your "Dumb" COVID Questions, Answered (Feb. '22 Edition)
Your "Dumb" COVID Questions, Answered (Feb. '22 Edition)
From immunity, to boosters, to the latest data — Dr. Jeremy Faust is here to give us the COVID-19 update.


So, here we are.
It’s February.
And Omicron is still with us.
It’s the bad houseguest who won’t leave, no matter how many hints you drop.
So many questions.
Time to check in with Dr. Jeremy Faust.

Photo courtesy: Dr. Jeremy Faust
Top ER doctor and Harvard educator.
What do you do once you’re infected? What’s the latest data on boosters? What kind of immunity can you expect from Omicron?
And the question we all ask ourselves daily: what am I comfortable doing in the midst of a global pandemic?
SO, YOU GOT COVID — WHAT DO YOU DO NOW?
ALINA CHO: Let’s say you get COVID, you don't live alone. You don't want to give it to other members of your household, what's the best way to check if you're still contagious?
DR. JEREMY FAUST: By and large, if you got exposed or started having a symptom, you got diagnosed, just wait five days. If you're getting better, then start using rapid tests after that point. My personal belief is, if you have two negative [rapid] tests, 24 hours apart, after [five days] and you're feeling well, then you're highly unlikely to be contagious anymore.

ALINA CHO: What about PCR tests? Let's say you tested positive, and you just want to know, "I don't have COVID in my system anymore." When can you safely PCR test and have a reasonable expectation that it will come back negative?
DR. JEREMY FAUST: Sometime in two or three weeks for most people, some people are even shorter than that, but if you retest a bunch of people at 20 days, you're going to find positivity. And the reason for that is, it's kind-of like rubble, you're find the finding the remnants of the virus's genetic code. This is what the PCR test does, it just finds the genetic code. So yeah, I'd say two or three weeks later, but generally, I wouldn't recommend using PCRs that way. I think the way to do it is to use PCR to diagnose the infection, and use rapids to diagnose when you're contagious.
ALINA CHO: Got it.
DR. JEREMY FAUST: And basically, unless you're extremely immune compromised, you can be pretty sure that the virus is out of your system within a couple of weeks.
THE LATEST DATA ON BOOSTERS
ALINA CHO: What about boosters? As we move forward, what do you sense that the booster situation might be like for, say, someone like me who got two Pfizer shots and a Pfizer booster?

DR. JEREMY FAUST: I think that the average person who has two doses and a booster has very little to fear in terms of severe outcomes. I've just never seen a patient do poorly who fits that description. I have seen patients who've been boosted do poorly who had advanced cancer and who essentially didn't have an immune system that could generate a response to the vaccine in the first place.
ALINA CHO: Right.
DR. JEREMY FAUST: For most people, two doses provide a ton of protection against severe disease. For people over 50 or so, a third dose adds genuine protection against severe disease.
ALINA CHO: Okay.
DR. JEREMY FAUST: That being said, I just want to say one thing. I think we finally now are starting to see more data about the safety of boosters, which we really didn't have, right? Because when we started rolling out boosters in September, we had like a month of data, and it was incomplete.
ALINA CHO: Right.
DR. JEREMY FAUST: Now finally, we're beginning to see the third dose safety in younger males, in particular, and it's reassuring. It's not as bad as the second dose, which is really what I was worried about, was that it would repeat the second dose in terms of rare events causing a rare [heart] condition called myocarditis.
ALINA CHO: Yeah.
DR. JEREMY FAUST: It turns out that the risk of myocarditis on the third dose is lower than the second dose, probably due to the spacing.
ALINA CHO: So that is an argument for boosters.
DR. JEREMY FAUST: It is. Yeah. I mean, I'll just tell you, I had not been boosted. Basically, I was waiting until the safety data was available. And it was pretty reassuring. So, I just decided that the risks are basically negligible.
ALINA CHO: So, did you get boosted?
DR. JEREMY FAUST: I did. Yeah.
WHAT ABOUT IMMUNITY FROM OMICRON?
ALINA CHO: Let's talk about immunity because there have been a few articles floating around out that suggest that you don’t get a lot of immunity from Omicron. Is that right?

DR. JEREMY FAUST: Overall, we need to reset our expectations on what we're hoping for in the future. I don't think we're hoping to eliminate infections because that will be impossible to achieve right now. I think what we're hoping for is for the infections to not mean as much, or to mean very little.
ALINA CHO: Exactly.
DR. JEREMY FAUST: So, for me, when I look at the data, it is possible that you don't get a ton of protection against reinfection from a new variant, and Omicron could turn out to be such a variant, but that doesn't mean that your next go-around, you didn't get some degree of continued protection or even enhanced protection against serious consequences.
ALINA CHO: That’s encouraging.
DR. JEREMY FAUST: There is data to show that vaccine plus infection is probably the best combination. Of course, getting to that point was dangerous, you had to get the virus.
ALINA CHO: Yeah, exactly.
DR. JEREMY FAUST: And you had to get lucky and not have anything bad happen. But once you've gotten there, you do have that going for you. So don't think that reinfection is going to be prevented by boosters that we have currently. But I think that these exposures, for better or worse, do add to our protection.
ALINA CHO: Individual and herd if you will, right?
DR. JEREMY FAUST: Yeah. In terms of the more feared long-term outcomes.
WHAT ABOUT DINING INDOORS, NON-ESSENTIAL TRAVEL?
ALINA CHO: In terms of comfort level, what are you comfortable doing right now? What are you not comfortable doing?
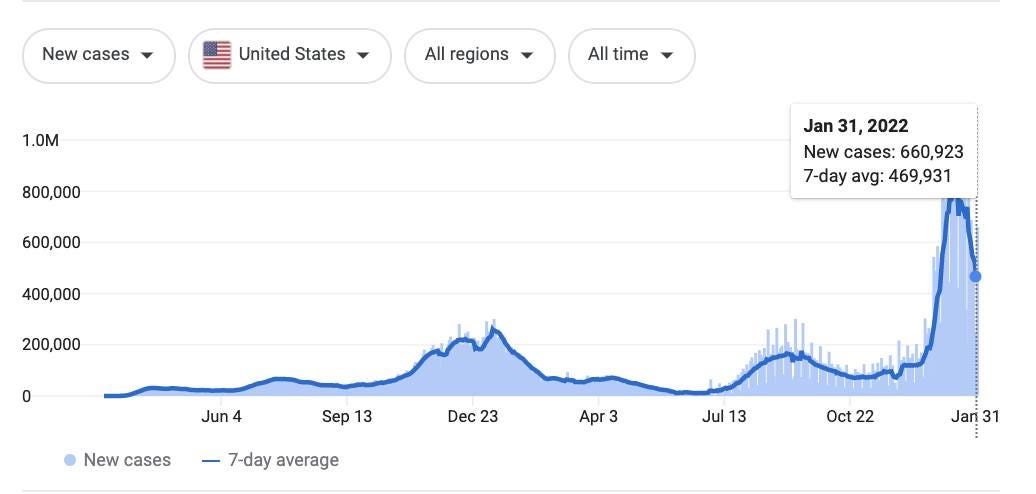
DR. JEREMY FAUST: I'm trying to think of how to frame this for you. When you look at the infection curves, the past month blew everything out of the water in terms of infections. It's just staggering, the number of infections that are out there, so when you play the math out, there's too much disease right now.
ALINA CHO: Even today, with all the reports of things waning?
DR. JEREMY FAUST: Oh yeah, because we're still above what we previously would've called absolute crisis, right?
ALINA CHO: Right.
DR. JEREMY FAUST: My parents, who are in their seventies, were going to come out this week and I told them not to because it just didn't make sense to put them in the airport, thousands of people, when maybe in a month, or a couple of weeks, the risk will be a tenth of what it is now. And so, it's just so astronomically high, the risk right now, that I've been holding off on things.
ALINA CHO: Such as?
DR. JEREMY FAUST: Dining indoors. Travel that's not essential. That kind-of thing. So yeah, I never catastrophize, but I don't downplay. What I will say is, I think that it's reasonable to assume that this wave will end at some point relatively soon. And the risk is so tremendously high to some people right now that it makes sense to hold off.
ALINA CHO: Got it.
DR. JEREMY FAUST: I know you're tired, but probably it's worth doing something for a couple of weeks when the risk is ten times higher. Omicron has unfortunately made me pull back from what I was wanting to do, but I also think that...
ALINA CHO: Hope is on the horizon?
DR. JEREMY FAUST: It's likely a shorter-term risk, but the question is how short term, and no one knows that.
ALINA CHO: I mean, people are saying March, April, things could get better. Are you hopeful about that?
DR. JEREMY FAUST: Well, what I do is, I proceed as if it's possible.
ALINA CHO: Yeah.
DR. JEREMY FAUST: And prepare for it to be ruined. So, we're planning an event for our preschool and it's in April or May, and we'd love it to be indoors, and so we're going to proceed with that. But there's a reasonable chance that something might prevent that from happening. I think that the combination of seasonal effects, Omicron, more vaccinations, more boosters, things realistically could get better, and I can't wait for that. So, it's the old hope for the best, plan for the worst.